

Poor posture, unbalanced tight and weak muscles, stress, over training and joint dysfunction are all possible causes of low back pain. Frequently we see patients who may present with acute low back pain and sciatica.
Sciatica refers to back pain caused by a problem with the sciatic nerve. This is a large nerve that runs from the lower back down the back of each leg. When something injures or puts pressure on the sciatic nerve, it can cause pain in the lower back that spreads to the hip, buttocks and leg.
The most common symptom of sciatica is lower back pain that extends through the hip and buttock and down one leg. The pain usually affects only one leg and may get worse when you sit, cough or sneeze. The leg may also feel numb, weak or tingly at times.
The symptoms of sciatica tend to appear suddenly and can last for days or weeks.
Most people who get sciatica are between the ages of 30 and 50. Women may be more likely to develop the problem during pregnancy because of pressure on the sciatic nerve from the growing uterus and foetus. Other causes include a herniated or bulging disc and degenerative arthritis of the spine.

What is a bulging disc?
To understand what a bulging disc is, we must first understand the anatomy of the spine.
Put simply, the spine is made up of individual vertebrae stacked on top of each other. Between each vertebrae is an intervertebral disc that provides a cushion so the vertebrae don’t rub together.
The discs between the vertebrae have a gel like material inside (called a nucleus pulposus).
A great way to think of the discs is like that of a balloon filled with water – these discs help resist compressive forces on the spine.
When a disc bulges, the gel like material inside gets pushed back towards the nerves and structures of the spine. This bulge can sometimes compress nerves in your spine and cause pain, tingling / or burning sensation and / or other symptoms.
It is important to note that a bulging disc doesn’t always touch the nerves and, for many, a bulged disc doesn’t even produce any pain at all. However, it could progress to become a herniated disc eventually, which can be problematic.
What causes a bulging disc?
· Seated with poor posture for long periods of time.
· Repetitive bending, lifting and twisting, especially with poor form.
· Heavy lifting with poor form due to stress on front of spinal column causing disc to bulge out back.
· Can also result from osteoarthritis.
· Trauma such as a car accident.
How is a bulging disc different from a herniated disc and which is worse?
In most simple terms, a herniated disc is when the fluid material from the disc ruptures through the outer layer of the disc and now spills out. This material can directly compress on spinal nerves and spinal structures. If you use the water balloon example but now imagine the balloon has burst under pressure, that’s a herniated disc.
A bulging disc can be resolved over time if managed well, whereas the herniated disc will just scar down since the annulus (outer layer of disc) has ruptured.
A nice visual spine model is provided below differentiating between normal, bulging and herniated discs:
What are the symptoms of a bulging disc in the lumbar spine?
· Low back pain.
· Leg pain (not absolute).
· Decreased lumbar lordosis (lower back curvature becomes flattened – flatter lower back over time).
· Lumbar and hip muscle tightness.

 Wrist active range of motion, flexion and extension:
Wrist active range of motion, flexion and extension: Wrist stretch: Press the back of the hand on your injured side with your other hand to help bend your wrist. Hold for 15 to 30 seconds. Next, stretch the hand back by pressing the fingers in a backward direction. Hold for 15 to 30 seconds. Keep the arm on your injured side straight during this exercise. Do 3 sets.
Wrist stretch: Press the back of the hand on your injured side with your other hand to help bend your wrist. Hold for 15 to 30 seconds. Next, stretch the hand back by pressing the fingers in a backward direction. Hold for 15 to 30 seconds. Keep the arm on your injured side straight during this exercise. Do 3 sets. Forearm pronation and supination: Bend the elbow of your injured arm 90 degrees, keeping your elbow at your side. Turn your palm up and hold for 5 seconds. Then slowly turn your palm down and hold for 5 seconds. Make sure you keep your elbow at your side and bent 90 degrees while you do the exercise. Do 2 sets of 15.
Forearm pronation and supination: Bend the elbow of your injured arm 90 degrees, keeping your elbow at your side. Turn your palm up and hold for 5 seconds. Then slowly turn your palm down and hold for 5 seconds. Make sure you keep your elbow at your side and bent 90 degrees while you do the exercise. Do 2 sets of 15. Active elbow flexion and extension: Gently bring the palm of the hand on your injured side up toward your shoulder, bending your elbow as much as you can. Then straighten your elbow as far as you can. Repeat 15 times. Do 2 sets of 15.
Active elbow flexion and extension: Gently bring the palm of the hand on your injured side up toward your shoulder, bending your elbow as much as you can. Then straighten your elbow as far as you can. Repeat 15 times. Do 2 sets of 15.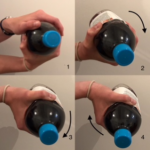 Eccentric wrist flexion: Hold a can, bottle or hammer handle in the hand of your injured side with your palm up. Use the hand on the side that is not injured to bend your wrist up. Then let go of your wrist and use just your injured side to lower the weight slowly back to the starting position. Do 3 sets of 15. Gradually increase the weight you are holding.
Eccentric wrist flexion: Hold a can, bottle or hammer handle in the hand of your injured side with your palm up. Use the hand on the side that is not injured to bend your wrist up. Then let go of your wrist and use just your injured side to lower the weight slowly back to the starting position. Do 3 sets of 15. Gradually increase the weight you are holding.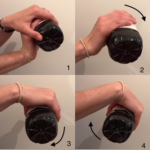 Eccentric wrist extension: Hold a can, bottle or hammer handle in the hand of your injured side with your palm facing down. Use the hand on the side that is not injured to bend your wrist up. Then let go of your wrist and use just your injured side to lower the weight slowly back to the starting position. Do 3 sets of one and gradually increase the weight you are holding.
Eccentric wrist extension: Hold a can, bottle or hammer handle in the hand of your injured side with your palm facing down. Use the hand on the side that is not injured to bend your wrist up. Then let go of your wrist and use just your injured side to lower the weight slowly back to the starting position. Do 3 sets of one and gradually increase the weight you are holding. Forearm pronation and supination strengthening:
Forearm pronation and supination strengthening: Wrist radial deviation strengthening: Put your wrist in the sideways position with your thumb up. Hold a can, bottle or a hammer handle and gently bend your wrist up. Do not move your forearm throughout this exercise. Do 2 sets of 15.
Wrist radial deviation strengthening: Put your wrist in the sideways position with your thumb up. Hold a can, bottle or a hammer handle and gently bend your wrist up. Do not move your forearm throughout this exercise. Do 2 sets of 15. Wrist exension with broom handle: Stand up and hold a broom handle in both hands. With your arms at shoulder level, elbows straight and palms down, roll the broom handle backward in your hand. Do 2 sets of 15.
Wrist exension with broom handle: Stand up and hold a broom handle in both hands. With your arms at shoulder level, elbows straight and palms down, roll the broom handle backward in your hand. Do 2 sets of 15. Grip strengthening: Squeeze a soft rubber ball and hold the squeeze for 5 seconds. Do 2 sets of 15.
Grip strengthening: Squeeze a soft rubber ball and hold the squeeze for 5 seconds. Do 2 sets of 15. Resisted elbow flexion and extension: Hold a can of soup with your palm up. Slowly bend your elbow so that your hand is coming toward your shoulder. Then lower it slowly so your arm is completely straight. Do 2 sets of 15. Slowly increase the weight you are using.
Resisted elbow flexion and extension: Hold a can of soup with your palm up. Slowly bend your elbow so that your hand is coming toward your shoulder. Then lower it slowly so your arm is completely straight. Do 2 sets of 15. Slowly increase the weight you are using.